

Mohan Singh, 52, was extremely anxious after discovering he had a 60% blocked heart artery. What confused him even more was that his friend, who had an 80% blockage, was not advised to get a stent, while he was.
This leaves many people wondering: when do you really need angioplasty or a stent, and when can it be avoided?
If you have the same question, you are in the right place. In this blog, we will explain in the simplest way possible when do you really need an angioplasty and stenting, so you can make a more informed and confident decision for yourself or your loved ones.
What Is Angioplasty and Stenting?
Angioplasty is a minimally invasive procedure used to widen narrowed or blocked heart arteries.
Doctors insert a thin tube called a catheter through the wrist or groin and guide a small balloon to the blockage, which is then inflated to improve circulation to the heart.
Stenting is usually performed alongside angioplasty. A stent is a small mesh-like metal tube placed inside the artery after the balloon opens it. This holds the artery open so it doesn’t get narrowed again.
Angioplasty vs Stent: What’s the Difference?
The table below will help you clearly understand the difference between angioplasty and stenting.
| Feature | Angioplasty | Stenting |
|---|---|---|
| What is it? | A procedure used to open blocked or narrowed heart arteries | A small mesh-like tube placed inside the artery |
| Purpose | Improves blood flow to the heart | Keeps the artery open after angioplasty |
| How is it done? | A small balloon is inflated at the blockage site | The stent expands inside the artery and stays there permanently |
| Main Tool Used | Balloon catheter | Metal mesh tube |
| Is it done alone? | Often done together with stenting | Usually placed during angioplasty |
| Does it stay in the body? | No, the balloon is removed after the procedure | Yes, the stent remains inside the artery |
| Main Benefit | Opens the blocked artery quickly | Reduces the chances of the artery narrowing again |
| Common Use | During severe blockage or a heart attack | To support the artery after it has been opened |
When is angioplasty really recommended?
Doctors usually recommend angioplasty in situations where the blood supply is dangerously reduced, which can threaten a life or when symptoms like chest pain or shortness of breath become so severe that they start affecting everyday life.
-
During a Heart attack
If you are having a heart attack (STEMI, NSTEMI), time is muscle. A heart attack happens when an artery is completely blocked. In this case, angioplasty is the “gold standard” treatment. As StatPearls (NIH) confirms, angioplasty with stenting is the preferred treatment in these emergencies.
In this situation, doctors aim to open the blocked artery as quickly as possible, ideally within 90 minutes of arriving at the hospital, to restore flow of blood and reduce damage to the heart muscle.
2. Unstable Angina: Severe Chest Pain That Does Not Improve
Doctors divide angina into two types. Stable angina and unstable angina.
If you have chest pain that comes with physical or emotional exertion and lasts about five minutes or less, it is called stable angina.
According to Harvard Medical School, in most cases of stable angina, angioplasty and stenting are not necessary. For most people, lifestyle changes and medication control symptoms just as effectively as angioplasty and without the procedural risks.
If you have chest pain that occurs even at rest, doesn’t improve with medication or lifestyle changes, it is called unstable angina.
Angioplasty is recommended for unstable angina to improve your quality of life. It helps you walk, exercise, and live without constant pain.
3. Very High-Risk Blockages
Some heart artery blockages are more serious because they affect a larger portion of blood supply to the heart
For example:
- Left main coronary artery blockage: This artery supplies blood to a large part of the heart, so blockage here can be very dangerous.
- Multiple major artery blockages: When several heart arteries are blocked together, the heart may not get enough blood and oxygen.
- Critical narrowing affecting blood supply: If an artery becomes extremely narrow, blood supply to the heart can be severely reduced, increasing the risk of a heart attack.
These may need angioplasty or bypass surgery, depending on severity.
4. Abnormal Stress Test With Symptoms
A TMT (Treadmill Test) checks how well your heart works during physical activity.
Doctors may recommend angiography or a stent if the test shows-
- Significant ischemia on TMT: The test shows the heart is not getting enough blood during exercise.
- ST depression or major ECG changes during exercise: This may suggest reduced blood flow due to artery blockage.
- Chest pain during the TMT test: Symptoms appearing during exercise can indicate significant blockage.
- Severe breathlessness or fatigue on mild activity: The heart may be struggling to pump enough blood.
- Poor exercise tolerance: If the patient cannot continue the test for long because of symptoms, doctors may consider further treatment like angioplasty.
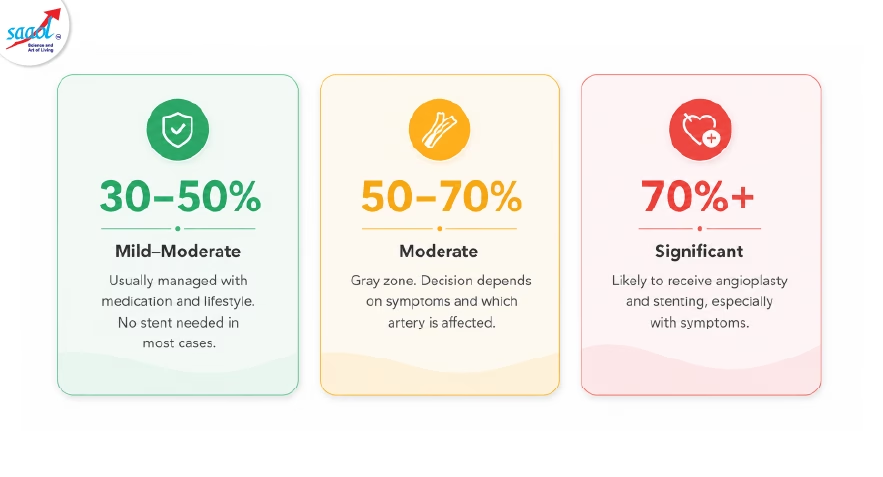
The “70 Percent” Rule: Is it Always Necessary?
You might hear a doctor mention a 70 percent coronary artery blockage. A 70% blockage means 70% of the artery’s diameter is narrowed by plaque.
In the medical world, a blockage of 70% or more in a major artery is often considered significant.
But you do not need to panic. The blockage percentage alone does not decide whether angioplasty is needed. The same 70% blockage may need a stent in one person, while in some cases it can be managed by medication and lifestyle changes. What matters more is how the blockage is affecting your heart’s function and your daily life.
Doctors also look at several other factors before deciding on angioplasty:
- Is the blockage causing symptoms?
Frequent chest pain, breathlessness, or fatigue may mean the heart is struggling to get enough blood. - Is circulation severely reduced?
If the blockage is significantly limiting blood supply to the heart, angioplasty may be needed. - Is the plaque stable or unstable?
Unstable plaque can suddenly rupture and trigger a heart attack, even if the blockage is smaller. - Is the patient diabetic?
Diabetes can make heart disease more aggressive and increase the risk of complications. - Are multiple arteries involved?
Several blocked arteries can reduce overall blood supply to the heart and may need more advanced treatment.
What Are the Risks of Angioplasty and Stenting?
Angioplasty is generally safe, but like any medical procedure, it carries real risks like-
Bleeding: The catheter insertion site (usually your wrist or groin) can bleed or bruise.
Blood Clot Formation: A clot can form inside or around the stent, especially in the first few months. This is why blood-thinning medications like aspirin and clopidogrel are prescribed immediately after the procedure.
Re-Blockage (Restenosis): The treated artery can gradually narrow again over time as scar tissue grows inside the stent. Drug-eluting stents significantly reduce but don’t fully eliminate this risk.
Kidney Strain from Dye: The contrast dye used during angiography is filtered through your kidneys and can temporarily strain them. People with pre-existing kidney disease face a higher risk of kidney damage.
Irregular Heartbeat (Arrhythmia): The catheter moving through heart vessels can briefly disturb the heart’s electrical signals. This usually resolves on its own but may require monitoring or medication.
Heart Attack or Stroke (Rare) In rare cases, a dislodged plaque fragment or clot can block an artery during the procedure, triggering a heart attack or stroke. This risk is low but is precisely why the procedure is done in a fully equipped cardiac lab.
Do Too Many Patients Get Unnecessary Angioplasty and Stents?
It might surprise you, but science shows that not every blockage needs a stent. While stents are lifesaving during a heart attack, they are sometimes overused in stable patients.
Major clinical trials (like the ISCHEMIA trial) have proven that for people with predictable chest pain, Optimal Medical Therapy, a combination of high-quality medicine and lifestyle changes, is often just as effective as a stent at preventing future heart attacks
Why does this happen?
- The “Fix-it” Instinct: Doctors often want to open a 70% blockage as soon as they see it on an angiogram.
- Symptoms vs. Survival: In stable cases, a stent is great for reducing heart blockage symptoms like chest pain, but it doesn’t always help you live longer than medicine alone would.
So, if it’s an emergency, it’s better to get the stent. If you are stable, ask your doctor if you can try medicine and lifestyle changes first.
A stent is a spot repair, but medicine treats your entire heart.
Can Blockages Be Managed Without Stenting?
Yes. In many stable patients, heart artery blockages can often be managed without a stent through medicines, lifestyle changes, and non-surgical therapies.
1. Medication & Lifestyle Changes
Doctors may first recommend:
- Cholesterol-lowering medicines
- Blood pressure and diabetes control
- Daily walking and exercise
- Weight loss
- Stress management
- Quitting smoking and alcohol
- A heart-healthy diet
These steps can help improve blood flow, control symptoms, and slow down further blockage buildup.
2. Additional Non-Surgical Support
For patients who need extra support beyond medicines, non-invasive therapies like EECP (Enhanced External Counter Pulsation) may also help.
How EECP Helps Manage Heart Blockages?
EECP (Enhanced External Counter Pulsation) is a non-surgical treatment that helps the heart get more blood naturally, without placing a stent or opening the chest.
Instead of mechanically widening one blocked artery, EECP improves overall circulation to the heart.
During the treatment, cuffs wrapped around the legs gently inflate and deflate with the heartbeat, helping push more oxygen-rich blood toward the heart.
Over time, this can help the body develop small alternate blood vessels, often called a “natural bypass,” which may improve blood supply around blocked arteries.
Because EECP is non-invasive, patients can usually continue their normal routine during treatment, making it a more comfortable option for many stable heart patients.

At SAAOL Heartcare, EECP is combined with lifestyle correction, diet management, yoga, stress reduction, and medical guidance.
To know more about our comprehensive heart care, consult the experts at SAAOL Heartcare today.
Book Appointment Call NowThe Takeaway
Heart disease is serious, and the right treatment decision can make a big difference to your life and the people who love you. Before deciding on angioplasty or a stent, always understand your condition properly, consider your symptoms and overall health, and don’t hesitate to take a second or even third opinion.
At SAAOL Heartcare Delhi, our experts focus on helping patients understand what treatment is truly right for them, based on their overall heart condition, lifestyle, and long-term health goals.
FAQs
Q1. Does every artery blockage need a stent?
Not necessarily. While stents are life-saving during heart attacks, stable blockages, even those around 70% can often be managed with “Optimal Medical Therapy.” Decisions depend on your symptoms, the location of the blockage, and whether medication alone can safely keep your heart healthy.
Q2. How is angiography done?
Done under local anaesthesia, a thin tube is guided through your wrist to the heart. Contrast dye is injected to reveal blockages on X-rays. You’ll stay awake and relaxed, feeling only a brief warm flush. The procedure takes 30–60 minutes, and most patients go home the same day.
Q3. How to put a stent in the heart?
Doctors insert a thin tube called a catheter through the wrist or groin and guide it to the blocked heart artery. A small balloon is inflated to open the blockage, and a mesh-like stent is placed inside the artery to keep the blood supply smooth.
Q4. How long does a heart stent last?
Modern stents are designed to stay inside the artery permanently. For many people, they work well for years, especially with proper medicines and lifestyle changes. However, some patients may develop re-narrowing inside the stent or new blockages in other arteries over time.
Q5. When is angioplasty recommended over bypass surgery?
Angioplasty is preferred for single or double blockages, especially in an emergency. Bypass surgery (CABG) is generally recommended when there are multiple complex blockages, blockage of the left main artery, or reduced heart function. Your cardiologist and a cardiac surgeon usually review the angiogram together to decide.
Q6. Is EECP a safe alternative to stenting?
EECP is an FDA-approved, safe, non-invasive alternative for many stable heart patients when performed under medical supervision. It can help improve blood circulation, reduce chest pain, and support patients looking for a non-surgical treatment option and enhanced long-term quality of life.